
Before anything else: this is an explainer, not an endorsement or a shopping guide. It has no ties to Core Peptides or to any company mentioned here, and it links to none of their storefronts. Every link goes to something checkable: FDA warning letters, peer-reviewed trials on PubMed, and StatPearls. Peptides that are compounded or prescribed are not FDA-approved finished drugs, and anything labeled “for research use only” is not approved for human use at all, full stop. Last reviewed June 2026.
Most people assume the biggest danger in the peptide market is a bad batch, some contaminated vial from a shady lab. That assumption turns out to be a little off. The real risk sits somewhere quieter: not in what’s added to a product, but in what’s missing around it. A missing conversation, a missing check, a missing piece of evidence, a missing phone number to call later. None of those announce themselves at checkout. That’s what makes them worth mapping out.
One thing worth saying plainly up front: this piece has no contamination report about Core Peptides to wave around, and it isn’t going to invent one. Core Peptides is a real retailer. Its own catalog labels every product “for research use only” and “not for human consumption.” That label is the whole story here, not a scandal about one company.
It helps to think of a peptide purchase as passing through four checkpoints: before you buy, when the vial arrives, while you’re using it, and if something goes sideways afterward. On the research-chemical route, all four checkpoints turn out to be empty.
Checkpoint one: nobody asks if this is a good idea for you
Before a vial ever ships, no one asks about a person’s medical history, current medications, or existing conditions. That’s the conversation a clinician has, the one that catches contraindications before they become a problem. Skip that conversation and the risk isn’t just “is this product okay.” It’s “is this product okay for me,” and there’s no way to know without someone trained to ask.
This gap is easy to miss precisely because nothing dramatic happens. The order goes through. The vial shows up. The missing screening never makes noise, it just sits there, quietly unaccounted for.
Checkpoint two: nobody can say what’s actually in the vial
This is the one worth sitting with the longest. Research chemicals aren’t reviewed by the FDA for identity, strength, quality, or purity. There’s no independent authority releasing each batch, no required outside certificate, and no recall system if something’s wrong. A certificate of analysis from a research-chemical seller is a document that seller chose to publish. It isn’t an independent guarantee, and there’s no practical way for a buyer to confirm it matches the vial in their hand.
So the honest answer to “do I know what’s in this?” is no, not “probably,” just no. Identity, strength, purity, all of it rests on trust in the seller rather than on any outside verification. That’s true across the whole category, Core Peptides included, not because anyone’s been caught doing something wrong, but because the category simply has no mechanism to check. If a regulated drug has a problem, there’s a system to pull it from shelves. Here, there isn’t. There’s just the buyer.
Checkpoint three: the evidence is thinner than the marketing suggests
This is the surprising one, mostly because the marketing sounds so sure of itself.
Take BPC-157, one of the best-selling peptides in this space. A 2025 systematic review published in the HSS Journal screened 544 articles and included 36. Of those, 35 were preclinical, and exactly one was a small clinical study. The authors found no clinical safety data in humans [C3]. That’s the entire human evidence base for a compound sold everywhere as though it were established.
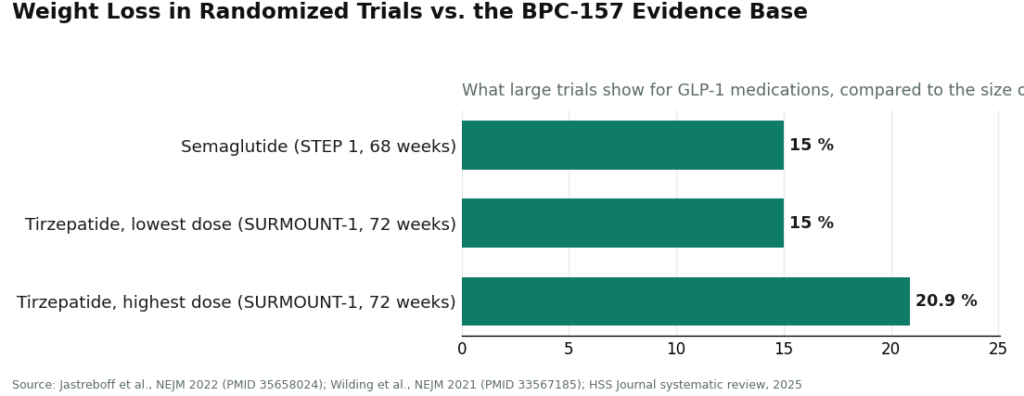
The contrast worth noticing is the metabolic peptides, which live in a completely different evidence universe. Semaglutide and tirzepatide work through the incretin system, suppressing glucagon, slowing gastric emptying, and increasing satiety [C6]. Semaglutide produced roughly 15% mean weight loss over 68 weeks in the STEP 1 trial [C5]. Tirzepatide produced 15.0% to 20.9% across doses over 72 weeks in SURMOUNT-1 [C4]. These are numbers from named, published trials, not from a lab notebook.
The gap between one small study and large randomized trials is the gap between something being studied and something being sold. The risk with peptides like BPC-157 isn’t that they’ve been proven unsafe. It’s that “nobody really knows yet” is being marketed as “safe and effective,” and those are not the same claim.
Checkpoint four: if something goes wrong, there’s no one to call
The last gap is the simplest. On the research-chemical route, the relationship ends at checkout. A reaction, a side effect, a worrying symptom, there’s no clinician on the other end of that. There’s a store that sold a laboratory chemical and disclosed, in writing, that it wasn’t meant for human use. That’s a disclaimer, not a support line.
A supervised route keeps someone in the loop, a clinician who can be reached, who can adjust a plan, who stays responsible after the sale. Without that loop, a side effect isn’t managed. It’s just faced, alone.
What the 2026 enforcement actions confirmed
Regulators appear to have landed on a similar conclusion. A September 2025 regulatory-law analysis documented more than fifty FDA warning letters aimed at compounded GLP-1 marketing and at “research use only” peptides advertised in ways that suggested human use, covering semaglutide, tirzepatide, retatrutide, BPC-157, and certain SARMs [C2]. Then on March 31, 2026, the FDA sent warning letters to peptide sellers including Gram Peptides, Prime Sciences, and Pink Pony Peptides, calling their products unapproved new drugs and stating that “evidence obtained from your website establishes that your products are intended to be drugs for human use” [C1].
Notice what the agency wasn’t warning about. It wasn’t flagging contamination. It was flagging the same missing structure described above: products sold as if for human use, without the screening, oversight, or follow-up that human-use products are supposed to carry. The “research use only” label, which a lot of buyers lean on as a kind of reassurance, was named as offering very little actual protection.
The honest caveat: supervised care isn’t risk-free either
Fairness cuts both ways here. A supervised route doesn’t erase risk. Peptide and GLP-1 medications carry real side effects. Compounded medications are not FDA-approved and haven’t been evaluated by the FDA for safety, effectiveness, or quality, and anyone claiming a compounded version is identical to the approved brand is overstating things.
FormBlends is one example of a supervised route, mentioned here once, not as a ranked recommendation. What it changes, structurally, is who’s in the room. A patient is connected with an independent licensed physician who writes the prescription, and the compounded peptides or GLP-1 medications are prepared by a state-licensed 503A pharmacy rather than a chemical supplier, across 47 states. That’s a description of the structure, not a sales pitch, and it doesn’t make risk disappear. It changes who’s managing it.
So the four checkpoints from earlier: the screening, the verified contents, the actual evidence, the follow-up contact. On the research-chemical route, all four are empty. On a supervised route, someone occupies each one, a licensed clinician, a licensed pharmacy, and an honest disclosure that “compounded” still means “not FDA-approved.” Neither path is magic. One of them just isn’t run alone.
Questions that come up a lot
What’s the biggest safety risk with research-chemical peptides?
It isn’t usually one bad vial. It’s the stack of missing pieces: no clinician checking for contraindications, no FDA review of identity, strength, or purity, no recall system if something’s wrong, and no follow-up if a reaction happens. These gaps are built into the “research use only” category itself, Core Peptides included, not because any one seller did something wrong, but because nothing in the category fills them.
Can a certificate of analysis from a research-chemical seller be trusted?
Treat it as a document the seller decided to publish, not an independent guarantee. It isn’t the same as FDA review or a recall-backed check, and there’s no practical way to confirm it reflects the vial actually received. Identity, strength, and purity all rest on trust in the seller, and trust isn’t verification.
Is BPC-157 safe?
Honestly, nobody can say with confidence, because the human data barely exists. A 2025 systematic review found no clinical safety data in humans for BPC-157, with 35 of 36 included studies being preclinical [C3]. The concern isn’t that it’s proven dangerous. It’s that it’s largely unstudied in people while being sold as though it were established. Unstudied and safe are not the same word.
Did Core Peptides do something dangerous?
No such claim is made here, and there’s no evidence for one. The documented 2026 FDA letters named Gram Peptides, Prime Sciences, and Pink Pony Peptides, among others [C1]. Core Peptides is mentioned only as a real research-chemical retailer whose catalog is labeled “research use only.” The risks discussed are structural to that whole category, not an accusation against one store.
Is the supervised route actually safe, then?
Safer, not risk-free, and it wouldn’t be honest to say otherwise. Peptide and GLP-1 medications carry real side effects, and compounded medications are not FDA-approved or FDA-evaluated for safety, effectiveness, or quality. What changes on a supervised route is who’s managing the risk, a licensed clinician and a licensed pharmacy, with the not-approved status disclosed rather than hidden. On the research-chemical route, no one is managing it at all.
What changed in 2026 that makes this more pressing?
The FDA put it on record that a “research use only” label doesn’t exempt a product marketed for human use from drug regulation. A September 2025 wave of more than fifty warning letters [C2] and the March 31, 2026 letters to peptide sellers [C1] both make clear the agency views these as unapproved drugs meant for people. The label a lot of buyers leaned on for reassurance turned out to carry very little weight.
What’s the best alternative to Core Peptides for someone who actually wants results?
It depends on the underlying goal. For someone with a genuine therapeutic need, a physician-supervised compounding pharmacy offers pharmaceutical-grade material, a real diagnosis behind the prescription, and someone accountable if something goes wrong. That’s a different category of product entirely from a research chemical, no matter how polished the packaging looks.
Is Core Peptides legit, or is it a scam?
“Scam” oversimplifies it. Core Peptides sits in the same legal gray zone as most research-chemical peptide vendors: products labeled not for human use, no FDA oversight on the finished goods, and purity that depends on third-party testing nobody outside the company can fully verify. That’s not fraud in the traditional sense, but it is a structure that puts all the risk on the buyer, which is worth knowing before ordering anything.
What do Core Peptides reviews actually tell you?
Mostly shipping speed, packaging, and whether someone felt something after using the product. They can’t say what was actually in the vial, what the long-term effects might be, or whether a good feeling reflects real biological action or a placebo response. Reviews are decent for judging customer service. They’re close to useless for judging safety or potency, and treating them otherwise is where people run into trouble.
Where should someone buy peptides instead of from Core Peptides?
A different research-chemical vendor doesn’t solve the underlying problem, it’s still an unregulated market either way. A genuinely accountable option runs through a licensed provider who can prescribe and a compounding pharmacy under state board oversight, like FormBlends, which operates within that physician-supervised model. It costs more and requires an actual consultation. That’s the point of it, not a drawback.
References
C1. FDA warning letters to research-peptide sellers (Gram Peptides, Prime Sciences, Pink Pony Peptides, and others), dated March 31, 2026; “research use only” and “not for human consumption” labeling does not exempt products marketed for human use, with the Gram Peptides finding reproduced. Policy Canary, April 2026. C2. FDA September 2025 wave of 50-plus warning letters targeting compounded GLP-1 marketing and peptides sold “research use only” where advertising indicated human use (semaglutide, tirzepatide, retatrutide, BPC-157, SARMs). Health Law Alliance regulatory analysis, 2025. C3. Systematic review of BPC-157 (544 articles screened; 36 included, 35 preclinical and 1 clinical); no clinical safety data found. HSS Journal, 2025. https://journals.sagepub.com/doi/abs/10.1177/15563316251355551 C4. SURMOUNT-1 tirzepatide trial: mean body-weight reduction 15.0% to 20.9% across doses at 72 weeks versus 3.1% on placebo. Jastreboff et al., New England Journal of Medicine, 2022. PMID 35658024. https://pubmed.ncbi.nlm.nih.gov/35658024/ C5. STEP 1 semaglutide 2.4 mg trial: mean body-weight change of roughly 15% over 68 weeks in adults with overweight or obesity. Wilding et al., New England Journal of Medicine, 2021. PMID 33567185. C6. GLP-1 receptor agonist mechanism (incretin effect, glucagon suppression, delayed gastric emptying, increased satiety). StatPearls, NCBI Bookshelf, Collins and Costello.




